
Hip Dips & the Gluteal Frame: Fat Grafting and Custom Hip Implants
Published June 1, 2026 · By Dr. Robert J. Troell, Board-Certified Facial Plastic Surgeon
Dr. Robert J. Troell, MD, FACS

The short answer: Hip dips are the natural inward depressions where the outer hip meets the pelvis — a normal feature, not a sign of weight. Most soft-tissue hip dips can be smoothed with enriched fat grafting, designed alongside the whole gluteal frame (narrowing the waist, building the upper curve); deeper, structural dips may need a custom hip implant. Below: how the frame is designed, candidacy, how long the result lasts, and recovery.
Two people can carry the same weight on the same frame and have completely different silhouettes. The difference is rarely size — it is the shape of the gluteal frame: where the waist narrows, where the hip carries volume, and whether the outer hip dips inward or curves outward. A Brazilian Butt Lift (BBL) is often described as "making the buttock bigger." In practice, the result patients respond to is usually a matter of contour: removing fat that flattens the frame, and adding fat where it builds the curve — including the hip dips.
This article focuses on the part of gluteal contouring that gets the least clear explanation online: hip dips and the lateral gluteal frame. It draws on Dr. Robert J. Troell's 2026 peer-reviewed study of 112 women who underwent VASER ultrasound-assisted liposuction with stem cell–enriched fat grafting to the buttocks and hip dips (Medical Research Archives, 14:4, DOI 10.18103/mra.v14i4.7467), and on his published work on aesthetic hip implants — a structural option for hip dips that fat alone cannot correct (Aesthetic Surgery Journal, 2022, DOI 10.1093/asj/sjac064). The figures above are averages from that 112-patient series and describe one surgeon's protocol; they are not a promise of any individual result. For readers weighing whether to store cells for future use rather than use them now, see Can you bank your own stem cells?
What this article covers: what the gluteal "frame" is and why shape beats size · what hip dips actually are · how fat grafting fills them · how fat removal and fat addition build an A-frame together · when fat is not enough and custom hip implants are considered · how much grafted fat survives · whether it is safe · candidacy · recovery · FAQ.
What the Gluteal "Frame" Is — and Why It Matters More Than Volume
Surgeons who specialize in body contouring describe the buttock not as an isolated structure but as a frame — the surrounding outline made by the lower back, the flanks (love handles), the outer hip, and the upper thigh. The aesthetic of the buttock is set as much by that frame as by the buttock's own projection. A narrow waist, a smooth outer hip, and a clean transition into the thigh read as a curved, lifted shape even when relatively little volume has been added.
The body-contouring literature commonly groups the female gluteal frame into four shapes: the A-shape (wider at the bottom — the most frequently requested), the round shape, the V-shape, and the square. In Dr. Troell's 2026 series, the desired frame was confirmed with each patient in advance, and the A-shape was the most common goal (DOI 10.18103/mra.v14i4.7467). Reaching it depends on three points along the side of the body: the upper outer hip, the mid-buttock, and the lateral (outer) thigh. Get those three points right, and the frame holds the shape.
This is why "how many cc's will you put in?" is the wrong first question. Two patients can receive the same grafted volume and look entirely different, because the frame — including whether the hip dips are addressed — determines how that volume reads.
Hip Dips, Explained: Why They Happen and Who Can Smooth Them
"Hip dips" — the inward depressions along the outer hip, just below the hip bone — are a normal feature of human anatomy, not a sign of being overweight or out of shape. They sit at the point where the outer edge of the pelvis meets the soft tissue of the upper thigh, over a depression near the greater trochanter (the bony prominence at the top of the thigh bone). Many people have them at every weight they have ever been, because their origin is partly skeletal: the width of the pelvis, the position of the hip bone, and the way muscle and fat drape over that structure.
That skeletal contribution is the key to understanding which hip dips respond to which treatment. Clinically, it is useful to separate two patterns:
- Soft-tissue-dominant hip dips. The depression is mostly a relative lack of fat and soft tissue over the outer hip, framed by fuller areas above and below. These tend to fill predictably with fat grafting.
- Structurally-dominant hip dips. The depression is driven more by the underlying bony anatomy than by a soft-tissue deficit. These can be softened with fat, but a deep, bony hip dip may not fully correct with fat alone — which is where a custom implant enters the conversation (covered below).
The distinction is made at consultation, using standing photographs in multiple views, palpation of the area, and a discussion of goals. There is no single answer that fits everyone — the honest version of this conversation includes telling some patients that fat grafting will improve a hip dip rather than erase it.
Fat Grafting to the Hip Dips, Step by Step
Hip-dip fat grafting is not a separate operation from a BBL — it is part of the same contouring session, because the fat used to fill the hip dips is harvested by the same liposuction that shapes the rest of the frame. In Dr. Troell's 2026 series, every patient who had buttock fat grafting also had hip-dip fat grafting, and a smaller group elected hip-dip transfer only (DOI 10.18103/mra.v14i4.7467). The sequence is:
- Harvest. Fat is removed with third-generation VASER ultrasound-assisted liposuction from areas that also improve the frame — lower back, flanks, and (commonly) the inner and outer thigh. Ultrasound energy is kept at a reduced setting to protect the fat cells that will be re-used.
- Process. The harvested fat is purified by centrifugation-filtration — spun and filtered to remove fluid, oil, and damaged cells — and enriched with the patient's own platelet-rich plasma (PRP) and adipose-derived stem cells. Roughly 60% of the raw harvested volume becomes usable, compacted, enriched fat.
- Place. Through small incisions at the lateral infragluteal fold (the crease where the buttock meets the thigh), the enriched fat is delivered into the subcutaneous plane only — above the muscle — in tiny 2–5 ml aliquots, with the cannula in motion, so each small parcel of fat sits close to a blood supply.
In the published series, the average compacted, enriched volume placed per hip dip was 45 cc (about 75 cc of raw harvested fat), compared with an average of 240 cc per buttock. Those are averages from one cohort, not a target every patient receives; the right volume is set by how much donor fat is available and how much the subcutaneous space will safely accept.
Why small aliquots matter. Grafted fat has no blood supply of its own for the first 1–2 days. It survives by absorbing oxygen and nutrients from the surrounding tissue until new vessels grow in. Many small parcels of fat have far more surface contact with that tissue than a few large boluses — which is why the technique emphasizes micro-aliquots placed while the cannula is moving, rather than large deposits.

Designing an A-Frame: It Is Built by Removing Fat as Much as Adding It
The most common misunderstanding about gluteal contouring is that it is purely additive. It is not. The curved, "heart-shaped" silhouette many patients describe is created as much by where fat is removed as by where it is added. Removing fat from the lower back and flanks narrows the waist and exposes the upper curve of the buttock; the outer hip and mid-buttock are then built up; and the result reads as an A-frame.
In the 2026 study, this was done in one 360-degree session: fat removed from the lower back, flanks, and frequently the inner and outer thighs to frame the buttock, then re-injected into the buttock and hip dips to build the curve (DOI 10.18103/mra.v14i4.7467). The lower-back and flank reduction is not optional polish — in the surgeon's description, framing those areas is what allows the buttock to read as lifted and projected. The female aesthetic the technique targets is often described as an inverted heart shape, with a small triangle of space defined between the inner thighs and the lower curve of the buttocks.
This is also why hip dips and buttock projection are planned together rather than separately. Filling a hip dip without addressing the waist and flanks can widen the silhouette instead of curving it; narrowing the waist without addressing the outer hip can leave the dip looking deeper. The frame is designed as one shape.
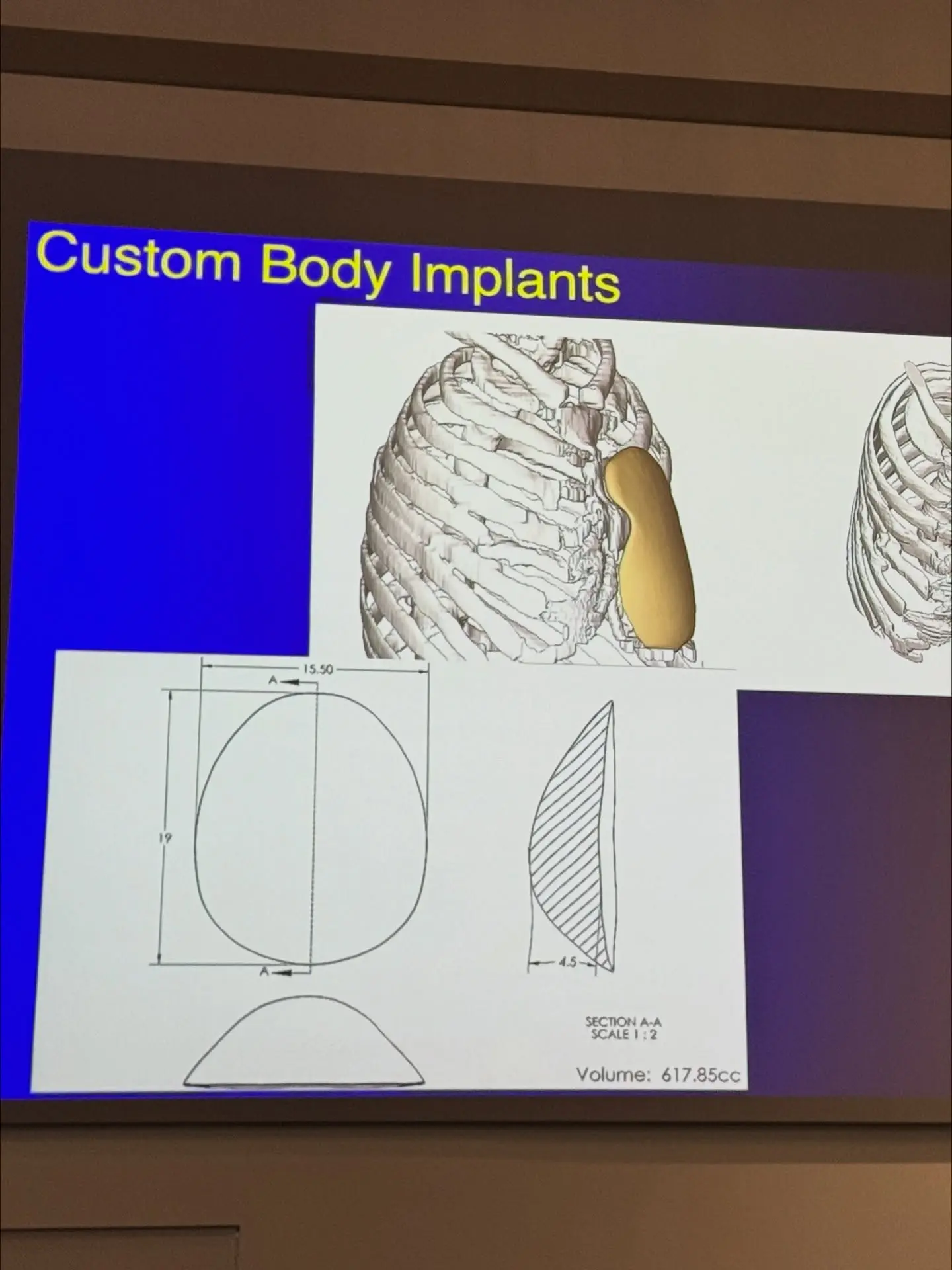
Custom Hip Implants for Structural Hip Dips
For most soft-tissue hip dips, enriched fat grafting is the first-line option — it uses the patient's own tissue, has no implant to maintain, and addresses the whole frame in one session. But some hip dips are structural: the depression is driven by the underlying bony anatomy, and there is a limit to how much a soft-tissue graft can fill a bony concavity. For those patients, fat alone may improve the contour without fully correcting it.
This is the part of hip and gluteal contouring where surgeon experience genuinely diverges, because aesthetic hip augmentation with custom implants is a niche within a niche — see our dedicated hip implants page for the full procedure. Dr. Troell is one of a small number of surgeons who have published peer-reviewed clinical work specifically on aesthetic hip implants — "Evolving Clinical Experiences in Aesthetic Hip Implant Body Contouring" in the Aesthetic Surgery Journal (2022, DOI 10.1093/asj/sjac064), co-authored with Barry Eppley, MD, DMD, and a second paper on hip-implant patient evaluation and implant fabrication. He has also taught hands-on body-implant cadaver courses, where the gluteal and hip vascular anatomy that governs safe placement is dissected directly.
In practice, three options are discussed for a structural hip dip:
- Enriched fat grafting alone — improves most hip dips; the first choice when the deficit is primarily soft-tissue.
- A custom (patient-specific) hip silastic implant — a more definitive correction for a deep, bony hip dip, designed to the individual's anatomy.
- Composite augmentation — an implant for the structural deficit combined with fat grafting to blend and refine the surrounding frame.
Which of these fits a given patient is a consultation decision based on photographs, palpation, the depth and origin of the dip, the amount of donor fat available, and the patient's goals. The point of naming all three is that a surgeon who only offers fat grafting can only offer a fat-grafting answer; addressing a structural hip dip well sometimes requires the implant option to be on the table.
How Much of the Grafted Fat Actually Stays?
The honest answer is that not all of it stays — and a good technique is built around that fact. Grafted fat that fails to establish a blood supply in the first days is reabsorbed by the body. The technique's job is to maximize the share that survives. Two numbers describe how this protocol approaches it:
- Processing yield. Centrifugation-filtration concentrates the harvested fat down to roughly 60% of its raw volume by removing fluid, oil, and damaged cells. What is injected is compacted, purified fat — so less volume is needed for the same result, and the injected fat is of higher quality.
- Retention. In the fat-grafting evidence and Dr. Troell’s clinical experience, roughly 75–85% of the grafted volume is retained at around seven months. Long-term data from Coleman shows that once grafted fat stabilizes — typically by 2–3 months — the surviving volume remains stable for years.
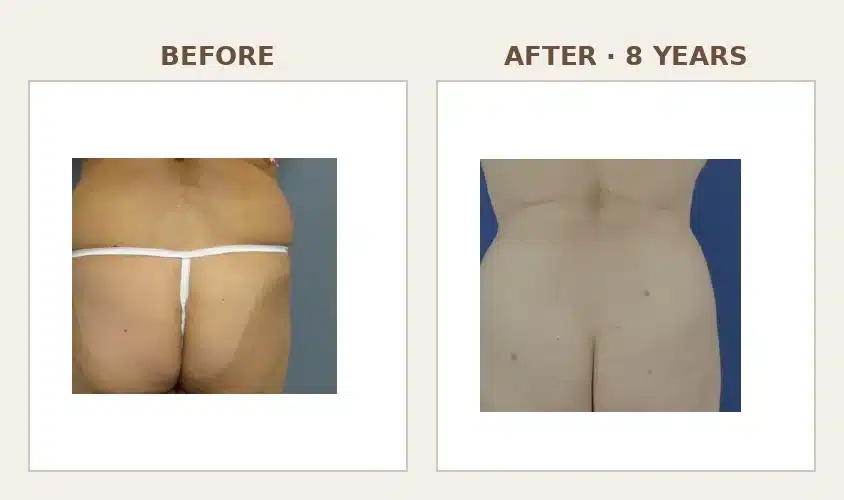
The PRP and adipose-derived stem cell enrichment is aimed squarely at this survival window: both promote the new blood-vessel growth (neovascularization) that determines which fat cells live past the first 1–2 days. It is also why the surgeon does not overfill — pushing more fat into the subcutaneous space than it can support raises the pressure on the grafted cells and lowers survival, the opposite of the goal. The durability of a well-executed graft is real: Dr. Troell has followed a patient with a maintained result at eight years.
Is Hip and Buttock Fat Grafting Safe?
BBL has historically been the most scrutinized procedure in aesthetic surgery because of a specific, serious risk: pulmonary fat embolism (PFE), which is tied to fat injected deep into the gluteal muscle. The protocol described here is built to avoid that mechanism — fat is placed in the subcutaneous plane only, never the muscle; the patient is awake enough to give immediate feedback if a cannula approaches the muscle; and intraoperative ultrasound is used to confirm the plane. In the 112-patient series, there were no pulmonary fat emboli, no oil cysts, and no anesthesia-related complications (DOI 10.18103/mra.v14i4.7467). The procedure still carries real risks — seroma, contour irregularity, infection, and the need for revision among them — and no single series guarantees outcomes for other patients or surgeons.
Because the safety mechanics deserve more than a paragraph, they are covered in full in a companion article: how awake anesthesia and subcutaneous-only fat grafting lower BBL risk — including the subcutaneous-plane rule, the published complication data, and the questions to ask any prospective surgeon. If you are weighing this procedure, read that article alongside this one.
Who Is a Good Candidate — and Who Is Not
Hip and gluteal fat grafting depends on two things the patient brings to the table: enough donor fat to harvest, and a realistic understanding of what reshaping the frame can and cannot do. A very lean patient may not have the donor volume for a large change; a patient well above their ideal body weight is usually advised to optimize weight first, both for safety and because the result is more stable at a steady weight.
In the 2026 protocol, candidacy and preparation included:
- Weight optimization. Patients were encouraged to be at or near their ideal body weight; those above it were counseled on a weight-loss trial before contouring.
- Medication review. Drugs that interfere with the liver enzyme that clears the local anesthetic (cytochrome P-450 inhibitors — certain antidepressants, blood-pressure medications, antifungals, and others) lower the safe anesthetic dose and are reviewed in advance.
- Hormone and GLP-1 timing. Oral estradiol was stopped at least two weeks before surgery to lower clot risk; GLP-1 weight-loss medications were stopped two weeks before as well.
- Smoking and vaping cessation. Stopping at least 2–3 weeks before and continuing after surgery to lower infection risk and protect fat survival.
Patients who request general anesthesia, who want a silastic gluteal or hip implant, or whose goals exceed what the subcutaneous space can safely hold in one session may be referred, staged, or counseled toward a different plan. Patient selection is itself part of the safety of the procedure — the favorable outcomes in any published series reflect, in part, who was chosen to operate on.
Recovery and Results Timeline
Recovery from hip and gluteal fat grafting is governed by one overriding principle: protect the newly grafted fat while it establishes a blood supply. That shapes most of the aftercare instructions.
- Sitting. Patients may sit, but are asked not to sit against the back of a chair — to avoid compressing the grafted fat — for a minimum of two weeks, preferably four to five. Sleeping on the stomach or sides is recommended for the same period.
- Compression and garments. A fitted compression garment is worn over the liposuction areas (not the buttock) continuously for about a month, then at night for an additional week.
- Lymphatic massage. Gentle massage of the liposuction sites is used to reduce swelling and fluid; this typically begins a few days after surgery.
- Activity. No vigorous exercise for several weeks to reduce the risk of seroma; no swimming or soaking until incisions are fully healed at about four to five weeks.
The shape continues to evolve as swelling resolves and the surviving fat stabilizes. A reliable estimate of the final volume is usually available around three months, and the result is stable thereafter — Dr. Troell has seen results maintained at eight years in his own patients. Patients who want more volume than a single session safely allows are offered a staged second graft no sooner than three months after the first.
Why a Published, Board-Certified Surgeon's Approach Matters Here
Hip and gluteal contouring sits at the intersection of two things that are hard to find in one surgeon: a safety-first liposuction-and-fat-grafting protocol, and genuine experience with the structural options — custom hip implants — for the hip dips that fat cannot fully correct. Dr. Robert J. Troell is board-certified in cosmetic surgery and in facial plastic & reconstructive surgery, with more than 30 years of surgical experience, and has published peer-reviewed work across this exact territory: the 2026 gluteal and hip fat-grafting series (DOI 10.18103/mra.v14i4.7467), the 2022 aesthetic hip-implant paper in the Aesthetic Surgery Journal (DOI 10.1093/asj/sjac064), and a body of liposuction and fat-grafting research spanning two decades.
That published record is not a marketing detail — it is the difference between a surgeon who follows the contouring literature and one who contributes to it. When you are choosing where to have a procedure as technique-dependent as this one, the substance of the consultation matters more than the size of the promise.
Hip Dips & Gluteal Frame Fat Grafting: Common Questions
What are hip dips, and can surgery fix them permanently?
Hip dips are the inward depressions along the outer hip, where the soft tissue of the upper thigh meets the bony edge of the pelvis over a natural hollow near the greater trochanter. They are a normal anatomical feature, not a sign of being overweight. Most soft-tissue hip dips can be smoothed with fat grafting, and the surviving fat is a stable, long-term result — Dr. Troell has followed a patient who maintained the outcome at eight years. Hip dips that are mainly structural (driven by the bony anatomy) can be improved with fat but may need a custom hip implant for a fuller correction. No procedure makes the underlying pelvic shape change, so "permanent" means the soft-tissue change is durable, not that anatomy is erased.
Fat grafting vs. hip dip filler vs. implants — which is right for me?
For most patients, enriched fat grafting is the first-line option because it uses your own tissue, addresses the whole frame in one session, and has no implant to maintain. Temporary injectable "hip dip filler" (hyaluronic acid or biostimulators) can soften a shallow dip but requires repeat treatment and is limited in volume. Custom hip implants are reserved for deep, structural hip dips that fat alone cannot fully correct, or for patients who want a more definitive, larger augmentation. The right answer depends on the depth and origin of the dip, how much donor fat you have, and your goals — which is what a consultation is for.
Will the fat in my hips stay, or will it disappear?
Some of every fat graft is reabsorbed in the first weeks, before the surviving fat establishes a blood supply. With centrifugation-filtration processing and PRP/stem-cell enrichment, in the fat-grafting evidence and Dr. Troell’s clinical experience roughly 75–85% of the grafted volume is retained at around seven months, and grafted fat that survives past 2–3 months tends to remain stable for years. Maintaining a steady weight matters — grafted fat behaves like the rest of your body fat, so significant weight loss can reduce it and weight gain can enlarge it.
Can I get an A-frame or "heart-shaped" result, or does my anatomy decide?
Both. The A-shape (heart-shaped) frame is the most commonly requested goal, and it is created by combining fat removal from the waist and flanks with fat addition to the outer hip and buttock. But your starting anatomy — pelvic width, where you store fat, skin quality, and how much donor fat is available — sets the realistic range. A good consultation shows you, with photographs and morphing, what shape is achievable for your frame rather than promising a shape from a photo of someone else.
How much does hip and buttock fat grafting cost?
Cost depends on the number of liposuction areas, whether hip dips and the buttock are both grafted, and whether skin-tightening or other steps are added — so it is quoted after an in-person consultation, not from a flat price list. For a detailed breakdown of how VASER lipo 360 and BBL pricing is built, see the VASER Lipo 360 & BBL cost guide. Troell Cosmetic Surgery is a cash-pay practice and can provide financing options through CareCredit and Alphaeon.
Is hip dip fat grafting done awake, and is it safe?
In Dr. Troell's protocol, the procedure is performed under awake, oral-sedation, super-wet tumescent anesthesia — the patient is comfortable but alert enough to provide the immediate feedback that keeps the injection cannula in the safe subcutaneous plane. Fat is never injected into the muscle, which is the mechanism behind the most serious BBL risk. The 112-patient series reported no pulmonary fat emboli and no anesthesia complications, though the procedure still carries real risks. The safety mechanics are covered in full in the companion article on awake, subcutaneous-only BBL safety.
What if I'm thin and don't have much fat to transfer?
Fat grafting needs a donor site, so very lean patients may not have the volume for a large change. Options include gaining a small, stable amount of weight before surgery to increase donor fat, staging the procedure over two sessions, or — for the hip dips specifically — considering a custom hip implant, which does not depend on donor fat at all. A consultation assesses how much harvestable fat you have across the typical donor areas (lower back, flanks, thighs) and what that realistically allows.
How long until I see my final hip and buttock shape?
Swelling resolves over the first several weeks, and some of the grafted fat reabsorbs during that time. A reliable picture of your final volume is usually available around three months, and the result is stable after that. You will be asked to protect the area early — not sitting directly against a chair back for two to five weeks, wearing compression over the liposuction sites, and avoiding vigorous exercise — because that early protection is part of how much fat survives to become the final shape.
Patient education. This article translates peer-reviewed clinical research for a general audience. It is not a substitute for an in-person consultation, an individualized risk assessment, or informed consent obtained directly from a treating surgeon.
- Last medically reviewed: 2026-06-01 by Robert J. Troell, MD, FACS
- Conflict-of-interest disclosure: This article describes techniques used by Troell Cosmetic Surgery & Facial Plastic Clinic and summarizes peer-reviewed studies authored by Dr. Troell. The practice has a direct interest in patients considering the procedures described.

Begin Your Journey with Dr. Troell
Schedule a complimentary consultation with Dr. Troell to discuss your goals, explore your options, and receive an honest, expert assessment. No obligation, no pressure.
Mon–Fri, 8:30 AM – 5:00 PM