VASER + Renuvion: Minimally Invasive Facelift Alternative for the Neck — A 58-Patient Study
Published May 17, 2026 · By Dr. Robert J. Troell, Board-Certified Facial Plastic Surgeon
Dr. Robert J. Troell, MD, FACS

The short answer: VASER liposuction removes fat and sculpts the face and neck while Renuvion (helium plasma plus radiofrequency) tightens the skin in the same session — together restoring a defined jawline and neckline without a lift, under local anesthesia. Below: how the combination works, who it suits, and recovery.
Tightening the lower face and neck has been one of the harder problems in cosmetic surgery. Manual liposuction removes fat but leaves loose skin behind. A traditional facelift tightens skin beautifully but requires incisions, dissection, and recovery on a scale most patients want to avoid for a focal jowl or submental complaint. The two energy-based technologies described in this article — third-generation VASER ultrasound liposuction and Renuvion helium-plasma skin tightening (HPT) — were developed to close that gap.
This article summarizes the technique, the results, and the safety profile from Dr. Robert J. Troell's 2025 peer-reviewed study with co-author Dr. Shahin Javaheri, published in The American Journal of Cosmetic Surgery. Fifty-eight adults presented specifically requesting lower-face and/or neck liposuction and underwent the combined VASER + Renuvion protocol under local anesthesia in two private practices. No general anesthesia. No serious adverse events. A revision rate of 6.9%.
What this article covers: why the face and neck need a different approach than body lipo · the technique step by step · why VASER first and Renuvion second · who is a candidate · how this differs from a traditional facelift · recovery · the 58-patient safety profile · what the procedure cannot do · commonly combined procedures · FAQ.
Why the Face and Neck Need a Different Approach
The aging lower face and neck has three overlapping problems: excess fat under the jaw and along the jowls, skin that has lost elasticity and no longer retracts on its own, and the underlying soft-tissue support of the deep facial compartments that thins with age. Removing the fat is the easy half. The challenge is the skin envelope above it.
The published baseline is that manual suction-assisted liposuction (SAL) alone produces only about 8% to 10% skin retraction at six to eight weeks, stabilizing at roughly 8% at one year. That is enough for a younger patient with very localized fat and good skin tone, but it is not enough for a patient who already has visible jowl skin laxity or platysmal banding in the neck. Aggressive superficial liposuction can push retraction higher, but it raises the risk of contour irregularities, post-operative skin laxity from over-resection, and full-thickness skin injury — tradeoffs that are particularly intolerable in the face and neck, where contour irregularities are immediately visible.
Two energy-based technologies were developed to bring more retraction to the procedure without those tradeoffs: ultrasound-assisted liposuction (UAL) and radiofrequency-assisted liposuction (RFAL). VASER — third-generation UAL — delivers vibration amplification of sound energy at resonance through a small probe that emulsifies fat selectively while sparing connective-tissue scaffolding. Renuvion is a more recent technology: a helium-based plasma device that delivers radiofrequency energy through ionized helium gas, contracting collagen in the fibroseptal network (FSN) without the bulk heating risk of older RF body-contouring systems.
Combined, they target each layer of the problem separately. VASER addresses the fat. Renuvion addresses the skin envelope. The protocol Dr. Troell published is the safe and reproducible way to layer them in one operative setting.
The Combined VASER + Renuvion Technique, Step by Step
The published protocol is performed under local anesthesia, supplemented by oral lorazepam (1–2 mg) and hydrocodone (5–10 mg) about thirty minutes before the start of the case if the patient elects sedation. Cephalexin 1 g and ondansetron 4–8 mg are administered preoperatively. No general anesthesia or intravenous sedation is required.
- Marking. The lower face and/or cervical area is marked with the patient upright. Anatomical landmarks — the inferior border of the mandible, the gonial notch (location of the marginal mandibular nerve crossing at the facial artery), and the areas of fullness in the jowls and submentum — are identified before the wetting solution is delivered.
- Wetting solution. Klein-type solution (diluted lidocaine + epinephrine + bicarbonate in lactated Ringer's) is delivered to the surgical sites through blunt infiltration cannulas using either tumescent or super-wet anesthesia technique. The wetting solution provides the local anesthesia — the patient is awake but comfortable on oral medication alone.
- Incisions. Small 11-blade incisions are placed in the post-auricular crease at the earlobe (and occasionally the anterior neck). Plastic round skin guards protect the incision edges from thermal injury during energy delivery.
- VASER ultrasound delivery. A grooved 3.7 mm ultrasound probe is passed through the wetting solution at 40% energy in pulsed mode. The face receives 3 to 4 minutes of energy per side; the neck receives 3 to 6 minutes. The probe is felt as "buttery" tactile resistance — the published technique calls for low resistance and easy passage to indicate adequate emulsification.
- Small-cannula liposuction. 2.0 and 3.0 mm vented liposuction cannulas are used to evacuate the emulsified fat. The published protocol cautions against avoiding the gonial notch (where the marginal mandibular nerve crosses) and against superficial over-resection that produces contour irregularities. The deep portion just under the mandibular border is addressed disproportionately to define an aesthetically pleasing acute cervical-mental angle.
- Renuvion (HPT) energy delivery. A 15 cm radiofrequency helium-plasma handpiece is introduced through the same incisions, delivering 70 to 80 Joules of energy at 1.5 to 3 L/min helium flow. Six passes are performed for each treatment area — three antegrade and three retrograde — with probe movement no faster than 3 cm/s. The pre-tunneling that ultrasound and liposuction already performed enables smooth, comfortable advancement of the RF handpiece.
- Evacuation and closure. External hand pressure evacuates residual helium gas and fluid through the incisions. The incisions are closed; a bulky compression dressing is applied.
The published energy parameters in one place:
- VASER: 3.7 mm grooved probe, 40% energy, pulsed mode, 3–4 min face / 3–6 min neck per side
- Liposuction cannulas: 2.0 and 3.0 mm vented (low-trauma)
- Renuvion (HPT): 70–80 J energy, 1.5–3 L/min helium flow, 6 passes per treatment area, probe speed ≤3 cm/s
- Anesthesia: tumescent or super-wet local, optional oral lorazepam + hydrocodone, preop cephalexin + ondansetron
- Postoperative: bulky compression dressing 1–2 days, then Velcro compression garment continuously for 1 week and at night for 1–2 weeks
Why VASER First, Then Renuvion
The case for combining the two technologies is additive. Each contributes a different mechanism of skin retraction, and the combination produces a result neither can reach alone.
Manual SAL alone produces 8% to 10% skin retraction by inducing a low-grade non-thermal inflammation of the fibrocollagenous matrix that promotes neovascularization, neocollagenesis, and scar-tissue formation in the treatment plane.
Adding VASER ultrasound contributes another approximately 20% retraction on top of that baseline. The mechanism is mechanical stimulation of the fibroseptal network — the same scaffolding that holds the skin to the deeper structures — without thermal damage to the overlying skin. The Nagy and Vanek randomized split-body study comparing UAL versus SAL on opposite sides showed a 53% improvement in skin retraction on the UAL side at one year versus the 17% on the laser-assisted-lipo side.
Adding Renuvion (HPT) contributes additional skin retraction, with the published combination yielding measurably better skin tightening than UAL alone. The helium-plasma mechanism is different from older bulk-heating RF: helium is ionized at very low energy levels and the resulting plasma allows heat to be delivered to the fibroseptal network in two distinct ways — through the plasma beam itself and through joule-heating from the RF current passing from the electrode through the plasma to the patient. The treated tissue heats; the surrounding tissue stays cool. Because the FSN is the treatment target, there is no real focus on heating the overlying skin. Once the FSN contracts (collagen fibers shrink up to 65% when triple-helical collagen denatures from 290 nm to 105 nm), the overlying skin retracts and tightens.
Surface skin temperatures with bulk-heating technologies can reach 45°C and increase the risk of full-thickness skin injury. The Renuvion handpiece, by contrast, has been shown in a published animal study to raise external skin temperature no more than 3.6°C from baseline over the course of a typical six-pass treatment — with a maximum external tissue temperature of 43.3°C at the 80%-power, 4 L/min-helium setting. This is the safety margin that makes the combination feasible in the thin-skin anatomy of the face and neck.
Sequence matters. VASER is performed first because the emulsification and small-cannula liposuction pre-tunnel the tissue. The Renuvion probe then advances smoothly and comfortably through that pre-tunneled space. Without pre-tunneling, the helium gas flow can become obstructed at the probe tip and produce a brief automatic gas-flow shutoff (F13 error). With pre-tunneling, the antegrade and retrograde fanning pattern can be completed cleanly across all six passes.
Who the Combined Procedure Is For — and Who It Isn't
The published cohort enrolled adults between 24 and 66 years of age (mean 36) who presented specifically requesting lower-face (jowls) and/or neck liposuction. All participants were medically stable for an outpatient surgical procedure under local anesthesia. The fifty-eight patients across two clinical practices were consented to the implementation of UAL with HPT, including a discussion of the limitations of persistent excess skin, possible side effects, and complications.
Good candidates share a few traits:
- Discrete fat excess in the jowls, submentum, or anterior neck, with or without mild-to-moderate skin laxity
- Healthy enough for an outpatient procedure under local anesthesia
- Realistic expectations — the combination tightens skin substantially but does not reposition the SMAS or deep facial structures the way a deep-plane facelift does
- Stable weight — significant weight fluctuation after the procedure can affect the long-term result
- Non-smokers, or willing to abstain from smoking and vaping for 2–3 weeks before surgery and 2–4 weeks after
Patients who are less ideal candidates include those with severe skin laxity and platysmal banding who would be better served by a neck lift; patients with true SMAS ptosis requiring repositioning of the deeper facial soft tissues; patients on certain medications that interact with lidocaine through the cytochrome P-450 system; and patients with metallic implants in the head or neck that contraindicate radiofrequency energy delivery in that field.
How This Differs From a Traditional Facelift
The combined VASER + Renuvion procedure and a traditional facelift are not competing for the same patient. They are different operations that address different anatomical problems. The questions to ask are which problem the patient has, which approach fits their anatomy, and which recovery profile fits their life.
| Element | VASER + Renuvion | Traditional Facelift |
|---|---|---|
| Anatomical target | Subcutaneous fat + skin envelope (fibroseptal network) | SMAS, deep facial compartments, skin redraping |
| Incisions | Small post-auricular and occasionally anterior neck (4–5 mm) | Pre-auricular and post-auricular extending into hairline |
| Anesthesia | Local with optional oral sedation | General or deep IV sedation typical |
| Skin tightening mechanism | Fibroseptal network contraction (up to 65% collagen shrinkage) | Mechanical redraping after SMAS lift |
| Typical recovery | 1–2 days bulky dressing, garment 1–2 weeks, social downtime ~1 week | 2–3 weeks social downtime, full recovery 6–8 weeks |
| Best for | Discrete jowl or neck excess with mild-to-moderate laxity | Moderate-to-severe SMAS ptosis, deep nasolabial and jowl descent |
| Longevity | Multi-year result; depends on weight stability and aging trajectory | Long-lasting SMAS repositioning; visible 8–12 years |
For many patients, the right answer is one of the two. For some, the right answer is both — VASER + Renuvion is frequently combined with a midfacelift, facelift, neck lift, or chin implant in the same operative setting, as documented in the published series.
Recovery: Days, Weeks, and Months
Recovery is short by surgical standards but real. A bulky compression dressing is placed at the end of the operation and stays on for one to two days to prevent fluid collection and to keep the skin adherent to the contracting fibroseptal network beneath it. After the dressing comes off, a Velcro compression garment replaces it: worn continuously for one week and at night for an additional one to two weeks.
Expected clinical effects in the first weeks include mild discomfort, edema, ecchymosis, and itching. None of these were reported as serious in the published cohort. Patients were instructed to follow up at 1 day, 1 and 2 weeks, 1, 2, 3, and 6 months, and every year thereafter using the Global Aesthetic Improvement Scale (GAIS).
The visible skin-retraction improvement appears earlier than most patients expect — immediate contraction of the fibroseptal network occurs without heating the dermal full thickness, and that contraction is noted at the 24-hour postoperative visit. The retraction continues to improve over the first six months as collagen remodeling progresses, with the final aesthetic result stabilizing well beyond that point.
Most patients return to non-physical work within five to seven days, although bruising, edema, and the visible garment can shift that depending on the patient's social and professional context.
58 Patients, Zero Serious Adverse Events
Two patients (3.4%) reported no change. No patient reported a worse aesthetic outcome.
The complication with the most concern in any face/neck procedure is marginal mandibular nerve weakness, which appeared in seven patients (12%) as a temporary, unilateral lower-lip muscle weakness. The published protocol used a methylprednisolone (Medrol) dose pack to facilitate speed of recovery. All seven cases resolved completely within 1 to 6 weeks. None required surgical intervention.
Nine patients (15.5%) experienced minor contour irregularities; all but two resolved over several months spontaneously. The remaining two had persistent minor depressions in the jowl that were addressed with one syringe of dermal filler each. Two morbidly obese patients (3.4%) requested additional liposuction in a revision setting. The combined revision rate including both filler corrections and additional liposuction was 6.9%.
The five negative findings — helium embolism, deep or superficial burns, infection, hematoma, seroma, pigmentation change, increased healing time, scarring — were all reported as zero in the published series. Expected clinical side effects included mild discomfort, edema, ecchymosis, and itching, which are not adverse events.
Both surgeons (Dr. Troell and Dr. Javaheri) subjectively assessed skin retraction with the combination versus ultrasound alone and reported better skin tightening when HPT was added. The improvement was visible at the 24-hour postoperative visit and continued to improve over the first six months.
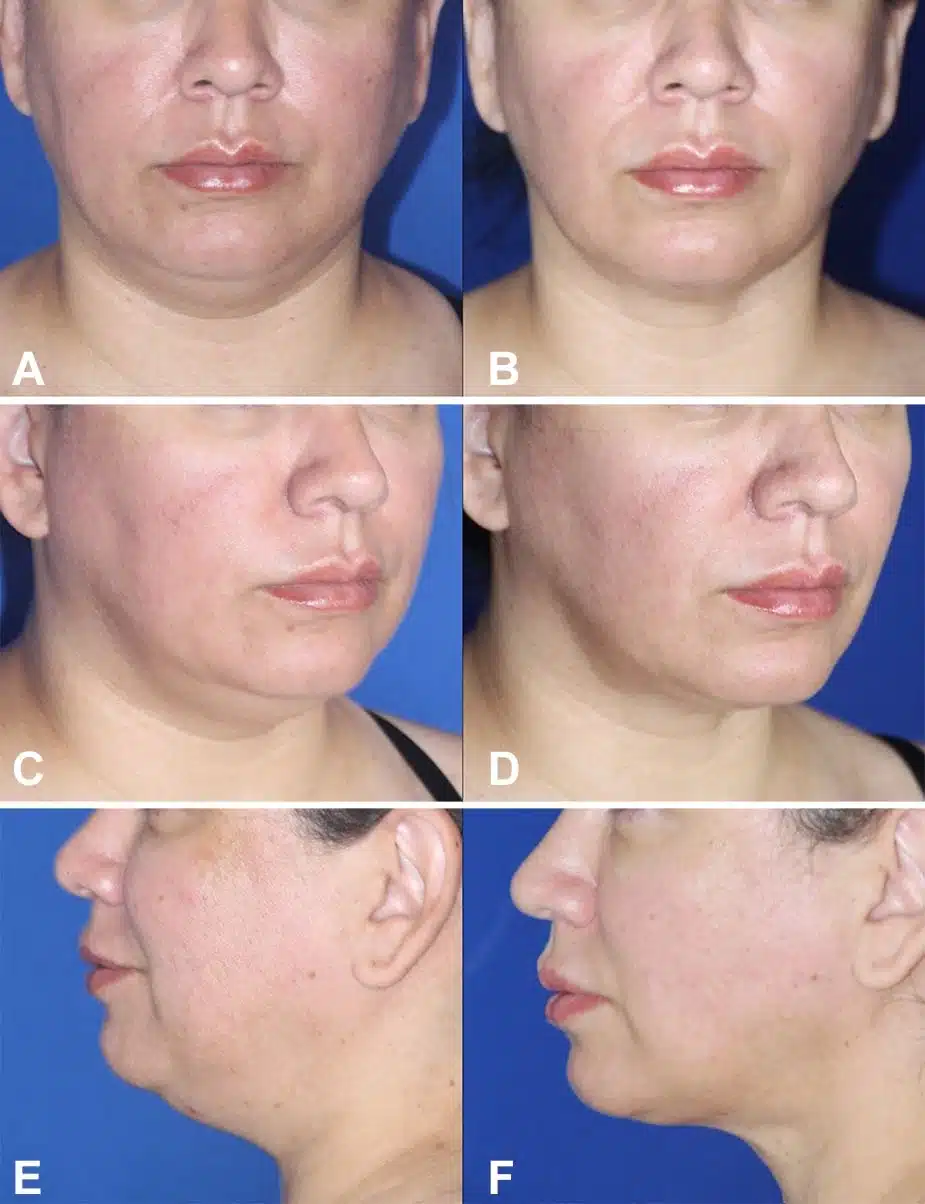
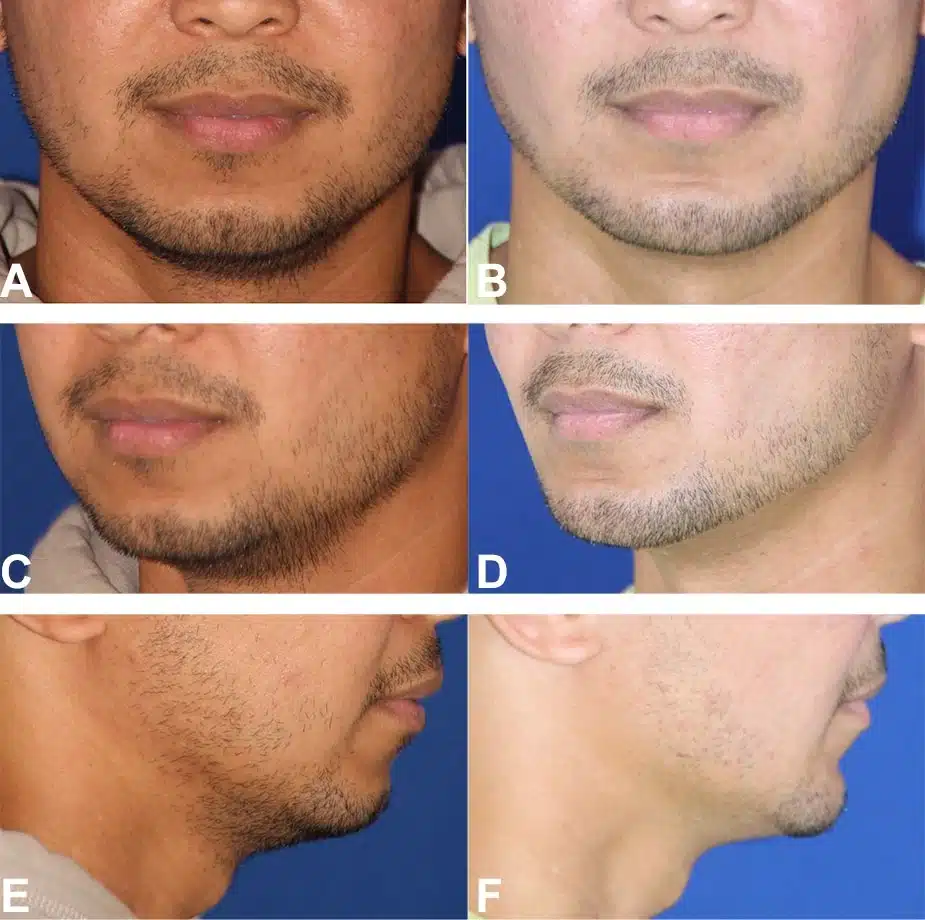
Real Patient Results from the 58-Patient Study
The following six figures are published in Combining Third-Generation Ultrasound Liposuction With Helium-Based Plasma Technology Skin Tightening in the Face and Neck (Troell & Javaheri, The American Journal of Cosmetic Surgery, 2025; DOI 10.1177/07488068251330030) and are republished here with patient consent. They show before-and-after results across the age range and procedure variations documented in the 58-patient cohort: lower-face-only, full face-and-neck, jowls-only, and combination presentations with adjunct procedures (blepharoplasty, midfacelift, chin implant).




Honest Limitations
The combined VASER + Renuvion procedure does several things very well. It also has limits the operator and the patient should understand before consenting.
- It does not replace a deep-plane facelift for severe ptosis. The procedure tightens skin and removes fat. It does not reposition the SMAS or the deeper facial soft tissues. A patient whose principal concern is the deep nasolabial fold or marionette descent of the lower face will not get a deep-plane-facelift result from this approach — even with maximum skin retraction.
- It does not address platysmal banding requiring direct correction. True platysmaplasty — the surgical correction of the central anterior neck band — is a different operation. Patients with prominent platysmal banding may benefit from VASER + Renuvion in combination with a neck lift that includes platysmaplasty.
- It does not address bony or volumetric deficits. A small or recessed chin contributes to the perception of a "double chin" that fat removal alone cannot fix. Patients with weak chin projection often benefit from a chin implant in the same operative setting.
- Result longevity depends on weight stability and the natural aging trajectory. Major weight gain or loss after the procedure can alter the contour. The skin tightening achieved is durable but not permanent against continued aging.
- It is not a weight-loss procedure. The published cohort enrolled patients who were medically stable for an outpatient procedure; two of the patients who later requested additional liposuction were morbidly obese. The procedure is a contouring operation, not a method of weight reduction.
Setting honest expectations during the consultation is the single most reliable predictor of patient satisfaction at six months. The 95.5% satisfaction rate in the published series was achieved in part by selecting the right patients and by setting the right expectations during the consent process.
Combined Procedures
The published case series notes that midfacelift, facelift, neck lift, and facial implants (midface or chin) are procedures commonly combined with face and neck liposuction. The combinations are not arbitrary — each addresses a layer the VASER + Renuvion procedure cannot reach on its own.
- Facelift / Midfacelift — for the patient whose principal concern is mid-to-deep facial soft-tissue descent rather than focal jowl or submental fat. Adding VASER + Renuvion to a facelift refines the skin envelope along the jaw and neck after SMAS repositioning.
- Neck Lift — for the patient with prominent platysmal banding or significant skin redundancy that cannot be tightened by HPT alone. VASER + Renuvion thins and tightens the surrounding skin; the neck lift addresses the platysma directly.
- Chin Implant — for the patient with a recessed or weak chin contributing to a poorly defined cervicomental angle. A silicone or extended anatomic chin implant placed through a submental incision in the same setting reshapes the lower-face profile (Figure 6 in the published series demonstrates this combination).
- Upper Blepharoplasty — for the patient whose upper-lid hooding distracts from the lower-face rejuvenation. The two procedures recover on overlapping timelines (Figure 5 in the series shows this combination).
- Facial Fat Grafting — the fat aspirated during the VASER liposuction can be processed and re-injected to add volume to deflated mid-face compartments. The same harvested fat that creates the jaw definition can restore mid-face volume in the same operative setting.
The decision to combine procedures is anatomical, not commercial. The right combination is the one that addresses every layer of the patient's actual concern in a single recovery period.
VASER + Renuvion FAQs
Is this a non-surgical procedure?
VASER + Renuvion is a minimally invasive surgical procedure. There are small (4–5 mm) incisions in the post-auricular crease and occasionally in the anterior neck. There is anesthesia (local, with optional oral sedation), an operating-room or surgical-suite environment, sterile technique, and energy delivery beneath the skin. It is meaningfully less invasive than a traditional facelift — no long incisions, no SMAS dissection, no general anesthesia — but it is not a no-incision treatment. Calling it “non-surgical” would be inaccurate.
How long until I can return to work?
Most patients return to non-physical work within five to seven days. The visible Velcro compression garment is worn continuously for one week. Bruising and edema in the lower face and neck typically resolve enough for routine appearances in seven to ten days. Vigorous exercise and physical activity are typically resumed at three to four weeks. Each patient is different; Dr. Troell reviews individual recovery expectations during the consultation.
Will I have visible scars?
The incisions for this procedure are 4 to 5 mm placed in the post-auricular crease and occasionally in the anterior neck. The post-auricular incision sits inside the natural skin fold behind the earlobe and is essentially hidden in everyday wear. The series of 58 patients reported zero cases of visible scarring as an adverse event.
What is the difference between Renuvion and other radiofrequency skin-tightening devices?
Older bipolar and monopolar radiofrequency-assisted liposuction (RFAL) devices work by bulk heating — the entire treatment volume is heated until a target temperature is reached, then maintained for a fixed time. Bulk heating drives skin-surface temperature up significantly (sometimes to 45°C) and increases the risk of full-thickness skin injury. The Renuvion helium-plasma mechanism is different: the device delivers radiofrequency energy through ionized helium gas, and the resulting plasma heats only the tissue surrounding the treatment area — the rest of the tissue cools rapidly. In the published animal study, external skin temperature rose no more than 3.6°C from baseline over the course of a typical six-pass treatment. That safety margin is what makes the technology useful in the thin-skin anatomy of the face and neck.
How much fat is typically removed?
Volumes in the published cohort ranged widely with the anatomy. Representative examples from the published figures: a 32-year-old patient had approximately 100 cc of fat removed (Figure 1); a 38-year-old had approximately 50 cc (Figure 2); a 40-year-old had approximately 125 cc (Figure 3); a 46-year-old had approximately 125 cc (Figure 4); a 59-year-old had approximately 75 cc from the jowls only (Figure 5, no cervical treatment); and a 37-year-old male had approximately 35 cc with a simultaneous chin implant (Figure 6). The volume target is anatomical, not numerical — the goal is the defined cervical-mental angle and the smooth jawline, not a specific cc number.
Is this covered by insurance?
VASER + Renuvion for the face and neck is a cosmetic procedure and is not covered by insurance. Dr. Troell’s practice does not bill insurance for any procedure. Patient-financing options including CareCredit and Alphaeon are available; the consultation includes a written quote with all costs disclosed.
How does this compare to a Renuvion-only treatment?
Renuvion-alone treatments target skin laxity in patients who do not have significant submental or jowl fat to remove. They are appropriate for the patient whose only complaint is skin looseness with minimal underlying fat excess. The published combination treats the two problems together: VASER removes the fat that defines the contour, and Renuvion tightens the skin envelope above it. Patients with both fat and skin laxity get a substantially better aesthetic result from the combination than from either treatment alone.
Will I need a facelift later?
It depends on the trajectory of aging and on the patient’s anatomy. The VASER + Renuvion result is durable but not permanent against continued aging of the deeper facial structures — the SMAS, the deep mid-face compartments, and the supporting fascia all continue to descend with age. A patient who has this procedure in their 40s may later choose a traditional facelift in their 50s or 60s to address that deeper descent. Many patients have both procedures across their cosmetic timeline; the two are complementary rather than competing.
Cited Sources
- Troell RJ, Javaheri S. Combining Third-Generation Ultrasound Liposuction With Helium-Based Plasma Technology Skin Tightening in the Face and Neck. The American Journal of Cosmetic Surgery 2025. DOI: 10.1177/07488068251330030.
- Nagy MW, Vanek PF. A multicenter, prospective, randomized, single-blind, controlled clinical trial comparing VASER-assisted lipoplasty and suction-assisted lipoplasty. Plast Reconstr Surg 2012;129:681e–689e.
- Ruff PG, Vanek P, Nykiel M. Adverse events of soft tissue coagulation using helium-based plasma technology alone and in combination with ultrasound-assisted liposuction. Aesthet Surg J Open Forum 2022;4:1–10.
- Duncan DI, Roman S. Helium plasma subdermal tissue contraction method of action. Biomed J Sci & Tech Res 2020;31(2):24063–24068.
- Chen SS, Wright NT, Humphrey JD. Heat-induced changes in the mechanics of a collagenous tissue: isothermal free shrinkage. J Biomech Eng 1997;119(4):372–378.
- Ruff PG, Bharti G, Hunstad J, et al. Safety and efficacy of Renuvion helium plasma to improve the appearance of loose skin in the neck and submental region. Aesthet Surg J 2023;43(10):1174–1188.

Begin Your Journey with Dr. Troell
Schedule a complimentary consultation with Dr. Troell to discuss your goals, explore your options, and receive an honest, expert assessment. No obligation, no pressure.
Mon–Fri, 8:30 AM – 5:00 PM