
Stem Cell Breast Fat Grafting vs Implants: 15-Year Evidence by Robert J. Troell, MD, FACS
Published May 21, 2026 · By Dr. Robert J. Troell, Board-Certified Facial Plastic Surgeon
Dr. Robert J. Troell, MD, FACS

The short answer: Stem cell–enriched breast fat grafting uses your own fat — no implants — to enlarge and reshape the breasts naturally. In Dr. Troell’s 15-year, 118-patient experience it achieved 95.8% satisfaction with 75–85% volume retention and zero oil cysts. Below: how it compares to implants, candidacy, and the long-term evidence.
The most common question in breast augmentation is no longer just "implants or not" — it is whether fat transfer can deliver a durable, natural result without the long-term complications of a synthetic implant. The honest answer has always been limited by the same problem: fat grafting results were variable, and the volume that survived was unpredictable.
In August 2025, Dr. Robert J. Troell, MD, FACS published a 15-year, 118-patient clinical study in the peer-reviewed Journal of Clinical Medicine (DOI 10.3390/jcm14165607; PubMed ID 40869433) documenting a stem cell-enriched fat grafting protocol that addresses exactly that problem. This article summarizes what that study — his own published series — found, in plain language, and what it means for someone weighing fat transfer against implants.
About this study and its author. The findings on this page come from a single-author, peer-reviewed study: Troell RJ, Breast Augmentation in Body Contouring Using Autologous Stem Cell-Enriched Fat Grafting: Fifteen-Year Clinical Experience, Journal of Clinical Medicine 2025, 14, 5607. Dr. Troell is both the operating surgeon for all 118 cases and the sole author of the paper, which was conducted in his practice with Institutional Review Board approval through Touro University Nevada, where he is an adjunct professor in the Department of Surgery. It is open-access under a Creative Commons CC BY 4.0 license. Every outcome number below is drawn directly from that paper.
What the 15-Year Evidence Shows: Fat Grafting vs Implants
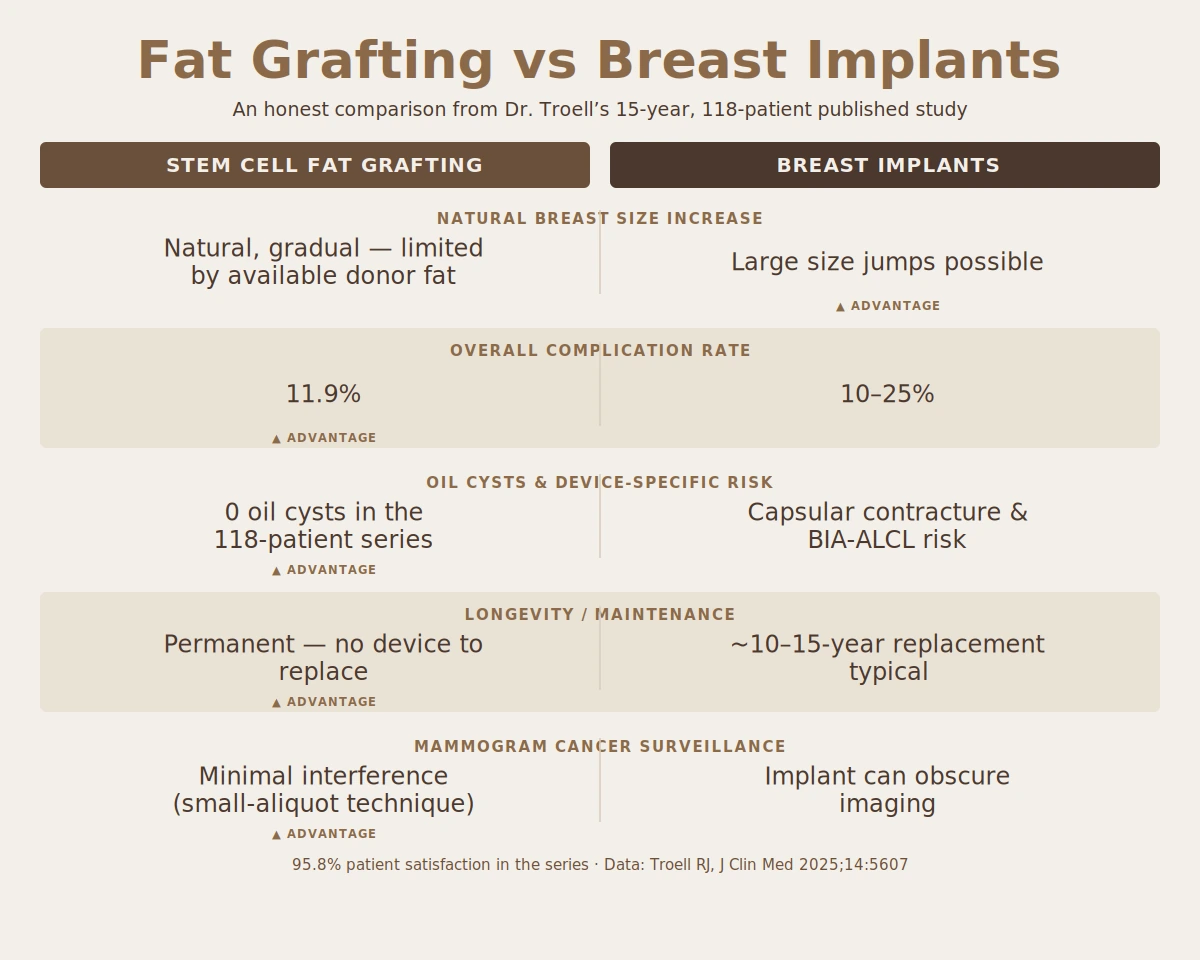
Across 118 consecutive women treated between 2008 and 2025 — the cohort Dr. Troell reported in his 2025 Journal of Clinical Medicine study — his stem cell-enriched fat grafting protocol produced consistent breast enhancement with a complication profile materially different from synthetic implants. That published series reports a 75–85% grafted volume take — the proportion of transferred fat that survives long-term — confirmed by a prior diagnostic 3D ultrasound measurement study. Patient satisfaction was 95.8% very satisfied or satisfied, with 4.2% dissatisfied (predominantly patients who wanted more volume than a single session delivered).
The most decisive comparison is the safety profile. Synthetic implants carry a reported long-term complication rate of 10–25%, including capsular contracture and the need for eventual revision or removal. In this 118-patient fat grafting series, the overall complication rate was 11.9% — and critically, there were zero cases of breast oil cyst formation, the complication most feared in fat transfer. The most common issue was seroma at the fat-harvest site (5.1%, six patients), followed by small palpable fibrotic areas (3.4%, four patients).
There is also a cancer-surveillance dimension that rarely gets discussed. Implants and poorly-performed fat grafting can both create calcifications that interfere with a radiologist's ability to read a mammogram. The study notes that meticulous fat grafting technique, distributing small fat aliquots rather than large pooled deposits, minimizes the macrocalcifications that obscure cancer surveillance — and cites evidence finding no increased cancer recurrence with adipose-derived stem cell breast fat grafting.
How Stem Cell Enrichment Actually Drives Fat Survival
This is the part most discussions skip. Patients hear "stem cell-enriched" and see the result — durable volume, no oil cysts — but the step in between is a black box. Here is what the biology actually does, drawn from the cellular-mechanism discussion in Dr. Troell's published 15-year study.
When fat is transferred, the grafted tissue has no blood supply of its own. For the first few days it survives only by diffusion from the surrounding recipient tissue. The grafted adipocytes (fat cells) at the center of a large deposit are too far from that supply and die — which is what produces fat necrosis and, eventually, oil cysts. The entire game is getting a new blood supply (neovascularization) into the graft before those cells starve.
Three elements of the protocol work together to win that race:
- Small fat aliquots, widely distributed. Instead of injecting large pooled deposits, the technique places many tiny fat parcels. Each parcel has a high surface-area-to-volume ratio, so every grafted cell is close to the recipient tissue's blood supply during the critical diffusion window. Smaller aliquots allow better neovascularization along the extracellular matrix scaffold.
- Adipose-derived stem cells (ASCs) and stromal vascular fraction (SVF). The enrichment step concentrates the support cells that keep the graft alive. Stem cells can survive 3 to 5 days on diffusion alone — long enough to bridge the gap until new blood vessels arrive — and they actively signal for that vessel growth.
- Platelet-rich plasma (PRP) and VEGF. PRP contributes roughly 30 blood-derived growth factors. The most impactful in fat transfer is vascular endothelial growth factor (VEGF), which stimulates new blood-vessel formation in the first 48 hours after grafting. PRP has been shown to increase adipocyte survival, multiply ASC numbers roughly four-fold, and build the fibrin matrix the new vessels grow along.
Put together: the small-aliquot delivery shortens the diffusion distance, the stem cells survive long enough to keep the graft viable and recruit vessels, and the VEGF in PRP accelerates the blood supply arriving. That is the chain that converts "transferred fat" into "surviving tissue" — and it is why this protocol reports a 75–85% volume take and no oil cyst formation rather than the variable, unpredictable results that gave fat grafting its earlier reputation.
Because this survival mechanism is biological rather than breast-specific, the same principles govern autologous fat transfer anywhere in the body. The identical small-aliquot, stem-cell-supported approach is what makes stem cell-enriched buttock fat transfer under awake anesthesia work as well — the destination tissue changes, but the biology that turns transferred fat into surviving, vascularized tissue does not.
Why the Harvesting Technique Decides the Outcome
Fat that is damaged during harvest cannot survive transfer, no matter how good the enrichment. The study is explicit that harvesting techniques which protect the adipocytes and avoid stem cell injury are the first determinant of graft survival. Gentle, low-pressure liposuction with the right cannula, the right wetting solution (lactated Ringer's is preferred over normal saline for adipocyte survival), and minimal processing trauma all preserve the living cells the graft depends on.
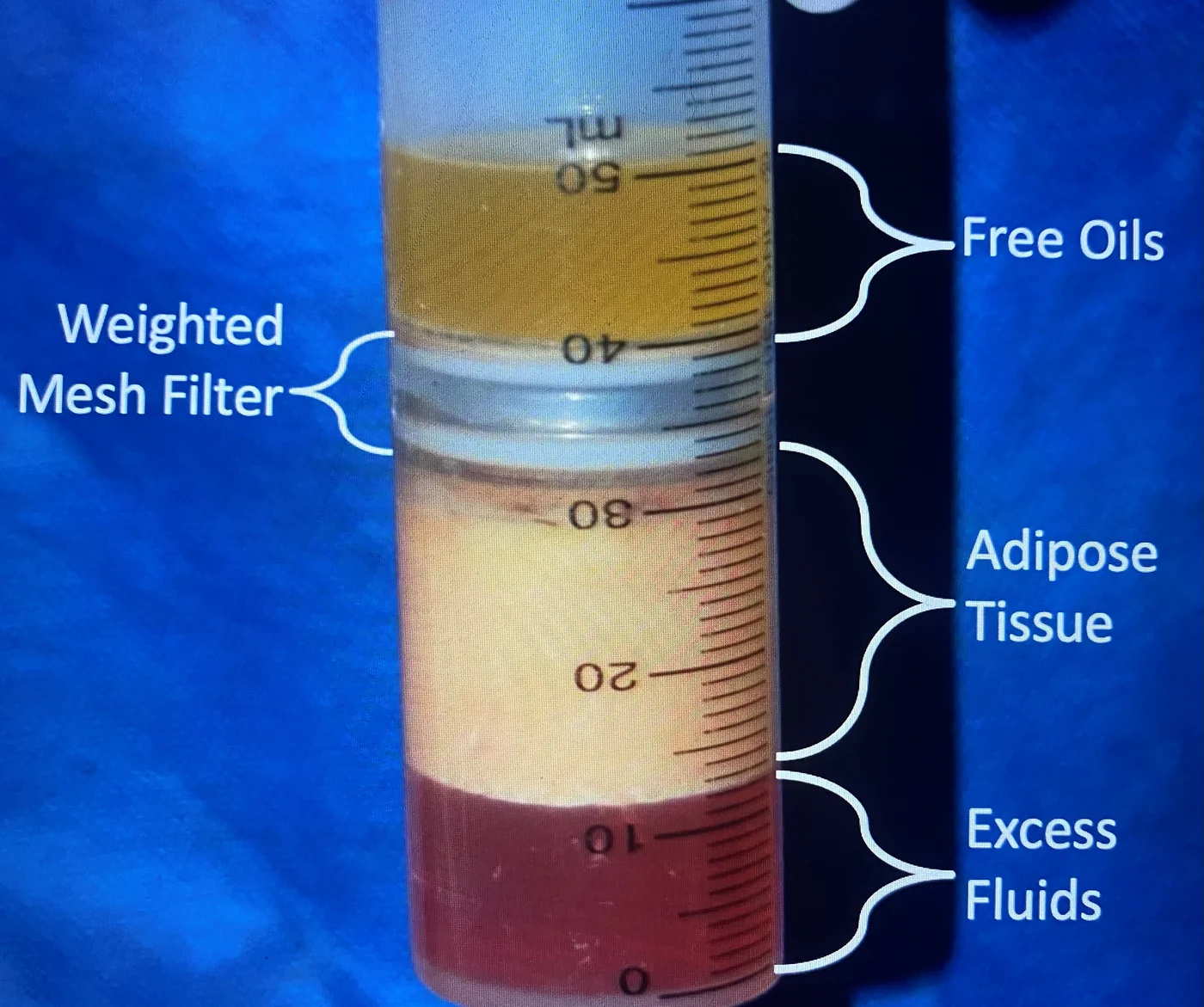
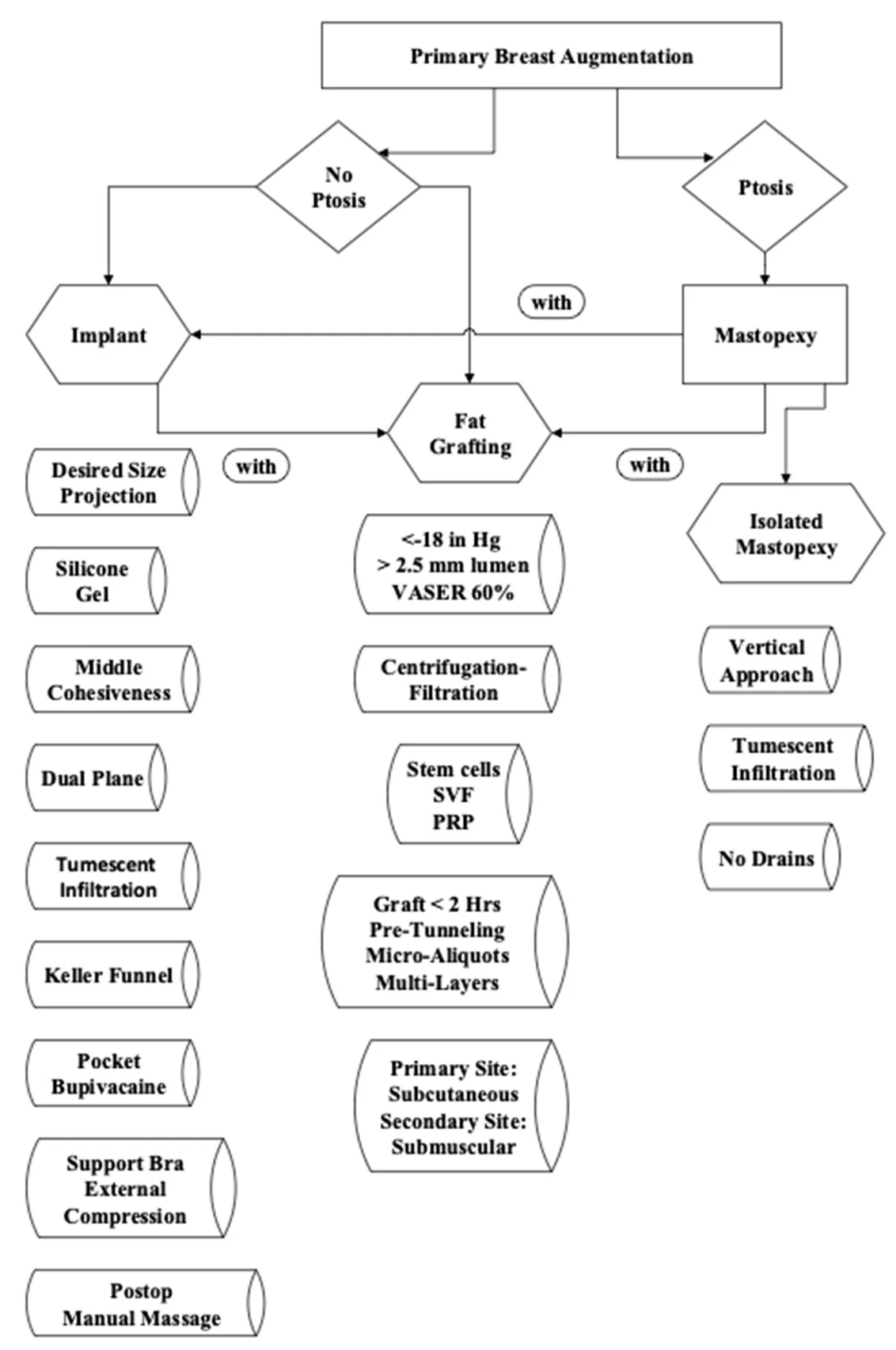
The harvested fat is then processed by centrifugation and filtration to concentrate the viable adipocytes and stem cells while removing oil, blood, and tumescent fluid — with minimal washing, because aggressive washing strips away the very growth factors that drive survival. In Dr. Troell's published protocol this purification step uses the patented MediKan TP-101 system — a weighted 60 cc syringe fitted with a 100-micron mesh filter that separates harvested fat into discrete layers (free oils above the filter, purified adipose tissue below, and excess fluids at the base). This is where the harvesting method matters: VASER ultrasound-assisted liposuction is the technique Dr. Troell uses to harvest fat with high cellular viability, and the canonical detail of how VASER works lives on its dedicated page. For the purposes of this study, what matters is that the harvest preserves the cells the enrichment step then concentrates.
The same VASER-plus-energy technique substrate appears across Dr. Troell's recent published work — including his 2025 study on combining VASER liposuction with Renuvion helium-plasma skin tightening for the face and neck. The harvesting discipline that protects fat for breast grafting is the same discipline that produces clean contour results elsewhere on the body.
Volume Retention: What "75–85% Take" Means Over Time
"Volume take" is the single number that decides whether fat grafting is worth it. Early fat grafting techniques lost so much volume so unpredictably that results were hard to promise. In Dr. Troell's 118-patient series, the mean volume of purified, enriched fat grafted was 192 to 206 cc per breast, with an estimated 75–85% volume take — the proportion of that grafted fat retained long-term — confirmed by a prior diagnostic 3D ultrasound measurement study rather than estimated by eye.
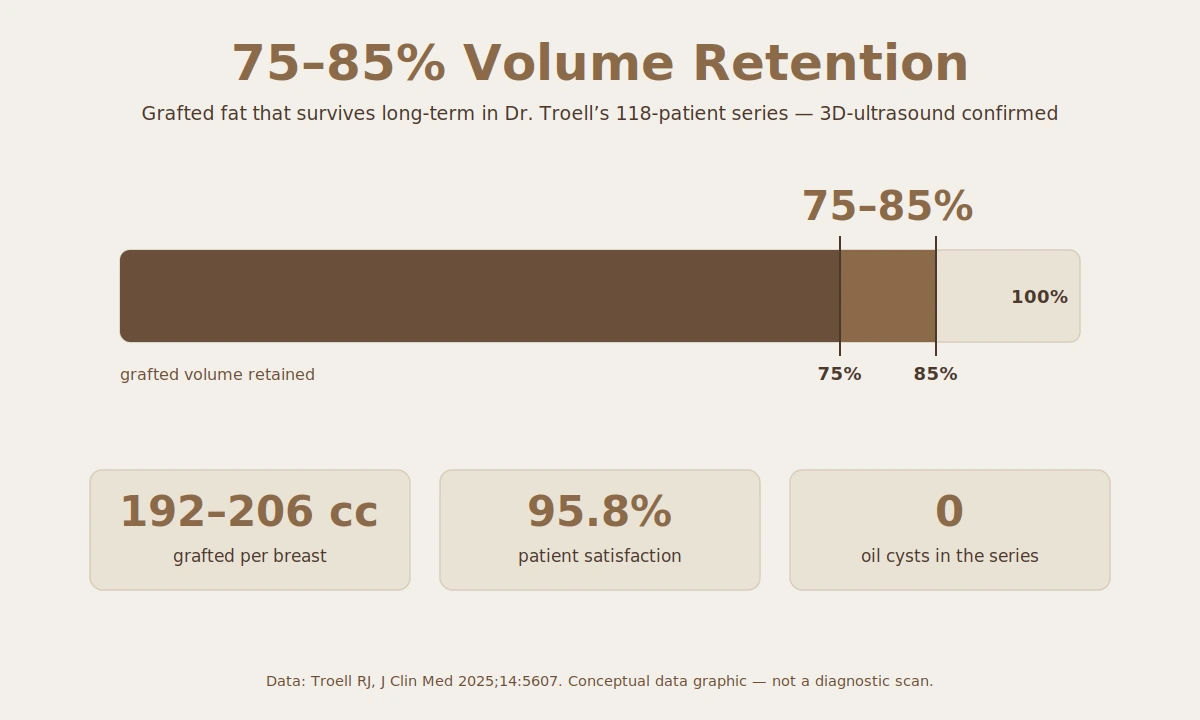
Retention matters for planning. Because the surviving fraction is high and consistent, most patients in the series needed only one fat grafting session; just 6.8% requested a second staged procedure to add further volume. That predictability — knowing roughly how much of the transferred fat will still be there a year later — is the practical payoff of the survival mechanism described above.
Complication Rate Across 118 Patients
The complication rate in Dr. Troell's 118-patient series — 11.9% overall — sits at or below the reported range for synthetic implants, and the nature of the complications is different. The most common was seroma (fluid collection) at the donor liposuction site, not in the breast itself. Palpable fibrotic areas occurred in four patients. The absence of any oil cyst formation across all 118 patients is the standout finding: oil cysts are the classic failure mode of fat grafting, and their elimination here is the direct downstream result of the survival mechanism — small aliquots and stem cell support meaning fewer fat cells die and pool.
One patient had a suspected atypical mycobacteria infection, and a small number of revisions were performed — almost entirely in patients whose only goal was augmentation and who wanted additional volume. These are the honest limits of any surgical series, reported transparently in the paper.
Is Breast Augmentation Without Implants Right for You?
The 118-patient population in Dr. Troell's study shows where stem cell fat grafting fits. The majority of cases — 65.8% — were primary breast augmentation for women who wanted a natural, modest size increase without a synthetic implant. The remaining cases were instructive: 13.6% were fat grafting after implant removal (women choosing to "go natural" after explant), 13.6% were performed during or after a breast lift or reductive mammoplasty, and 12.7% were combined with an implant exchange.
Good candidates generally share a few traits:
- A goal of natural, proportionate enhancement rather than a dramatic size jump — fat grafting adds volume gradually and within the limits of available donor fat.
- Sufficient donor fat to harvest (abdomen, flanks, thighs) — the procedure does double duty as body contouring at the harvest site.
- A preference to avoid synthetic implants and their long-term maintenance, capsular contracture risk, and eventual revision.
- Women considering explant who want to restore volume naturally after removing implants.
Ready to explore the procedure itself? The fat transfer breast augmentation service page covers candidacy, the published technique, cost factors, and recovery in Las Vegas.
Whether fat grafting, an implant, or a combination is right for a specific person depends on anatomy, donor fat, and goals. The breast augmentation procedure page covers the full range of options, candidacy, and what to expect — a decision finalized in consultation. This article's purpose is to explain what the 15-year evidence shows about the fat grafting option, not to prescribe one path.
Stem Cell Breast Fat Grafting FAQs
Is stem cell breast augmentation safer than implants?
In Dr. Troell's 118-patient, 15-year published series, the overall complication rate was 11.9%, at or below the 10–25% long-term complication rate reported for synthetic implants — with zero oil cyst formation and no implant-specific risks like capsular contracture. Fat grafting also avoids the implant-related calcifications that can interfere with mammogram cancer surveillance. "Safer" depends on the individual, but the published evidence shows a favorable, different risk profile.
How much fat volume is retained in breast fat transfer long-term?
The study reports an estimated 75–85% grafted volume take, confirmed by a prior diagnostic 3D ultrasound measurement study. With a mean of 192–206 cc grafted per breast and a high, consistent survival fraction, most patients (all but 6.8%) achieved their goal in a single session.
What is the complication rate of autologous fat grafting to the breast?
11.9% overall across 118 patients. The most common complication was seroma at the fat-harvest (donor) site at 5.1% (six patients), followed by small palpable fibrotic areas at 3.4% (four patients). There were no cases of breast oil cyst formation in the series.
Do stem cells prevent fat necrosis and oil cysts in breast grafting?
They are a major contributor. Fat necrosis and oil cysts happen when grafted fat cells die before a new blood supply reaches them. Adipose-derived stem cells survive 3–5 days on diffusion and signal for blood-vessel growth, while PRP-derived VEGF accelerates that vessel formation in the first 48 hours. Combined with small-aliquot placement, this is why the series reported zero oil cyst formation.
Can fat grafting replace implants for breast augmentation?
For the right candidate, yes — 65.8% of the series were primary augmentations with no implant, and another 13.6% were women restoring volume after implant removal. Fat grafting delivers natural, proportionate enhancement within the limits of available donor fat; it does not produce the large size jumps an implant can. The right choice depends on anatomy, donor fat, and goals.
What harvesting method is used for breast fat grafting?
Gentle, low-trauma liposuction that protects the adipocytes and stem cells, followed by centrifugation–filtration processing with minimal washing to preserve growth factors. Dr. Troell uses VASER ultrasound-assisted liposuction for harvesting; the technical detail of VASER lives on its dedicated procedure page.
Cited Source
- Troell RJ. Breast Augmentation in Body Contouring Using Autologous Stem Cell-Enriched Fat Grafting: Fifteen-Year Clinical Experience. Journal of Clinical Medicine 2025;14(16):5607. DOI: 10.3390/jcm14165607. PMID: 40869433. Open access, CC BY 4.0.

Begin Your Journey with Dr. Troell
Schedule a complimentary consultation with Dr. Troell to discuss your goals, explore your options, and receive an honest, expert assessment. No obligation, no pressure.
Mon–Fri, 8:30 AM – 5:00 PM